Types of Risk
The risk factors, ordered in terms of impact on all causes of Disability Adjusted Life Years (DALYs), in Somerset in 2019 are shown below.
The conditions that contribute to Global Burden of Disease Disability Adjusted Life Years (DALYs) indicate what needs to be treated. The risk factors suggest how the impact may be reduced or prevented. Key risk factors often affect multiple major causes of Disability Adjusted Life Years (DALYs). For example, smoking increases the risk of cardiovascular diseases like heart disease, stroke, and diabetes. It also impacts respiratory diseases like Chronic Obstructive Pulmonary Disease (COPD) and cancers such as lung cancer.
Secondary risk factors are those where early detection and treatment can improve outcomes. Encouraging healthier lifestyles can help reduce these behavioural risks. For environmental risks, we can work to reduce population exposure.
As with the priority health conditions, the importance of different factors is affected by classification, so, for instance, a single category of ‘diet’ would appear higher than the sub-category of ‘whole grains’. Other possible factors, such as social isolation or poor sleep, are not considered as risks in their own right.
Smoking (Behavioural)
Nicotine inhaled from smoking tobacco is highly addictive. It is the main reason people continue to smoke. But it is primarily the toxins and carcinogens in tobacco smoke, not the nicotine, that cause illness and death.
The best way for society to reduce these illnesses and deaths is to reduce the level of smoking in society to as low as practicable, which we achieve through tobacco control measures. The social patterns of smoking contribute to inequalities. Smoking prevalence is higher in so-called “routine and manual” workers and in people with mental health problems. Even though the data show long-term declines in the rates of smoking, the time lag between smoking and consequent conditions means that its impact continues to be significant.
Promoting smoke-free policies and services, supporting effective ways for people to stop smoking and to stop smoking when using or working in health settings can significantly improve the overall health of the population.
Key indicator: Smoking Prevalence in Adults in Routine and Manual Occupations (18 to 64) – current smokers (APS)
More smoking data from OHID Fingertips and Local Tobacco Control Profiles
High fasting plasma glucose (Secondary)
High blood sugar (hyperglycaemia) mainly affects people with diabetes and can be serious if not treated. A high level is usually considered to be over 7 mmol/L.
High blood sugar can signal a risk of developing type II diabetes. Identifying this risk allows for preventative measures, such as avoiding sugary or starchy foods, increasing exercise, reducing stress, and taking specific diabetes medications. Because it relies on medical tests, trend data or comparisons with England are not available.
High body mass index (Secondary)
Overweight and obesity occur when energy intake from food and drink consumption is greater than energy expenditure through the body’s metabolism and physical activity over a prolonged period. This results in the accumulation of excess body fat. However, there are many complex behavioural and societal factors that combine to contribute to cause this. Being obese or overweight can increase the risk of developing a range of serious diseases. The risks rise with BMI, and so are greater for obese individuals.
Overall, moderate obesity (Body Mass Index (BMI) 30 to 35 kg/m2) was found to reduce life expectancy by an average of three years, while morbid obesity (BMI 40 to 50 kg/ kg/m2) reduces life expectancy by 8 to 10 years. This 8 to 10 year loss of life is equivalent to the effects of lifelong smoking.
Key indicator
Hypertension (Secondary)
High blood pressure is an indicator of strain in the circulatory system, which can be related to behavioural factors such as diet, exercise or overweight. Like high fasting glucose, it shows how ill health can derive from many factors, and whilst genetics cannot (normally) be changed, there is often more than one way of reducing risk.
High blood pressure can also be treated medically as a way of averting more serious circulatory illness. Somerset has tended to show higher rates than the England average, and the rates have been rising. This reflects the relatively elderly population of the county, and may also indicate an effective programme of identifying hypertension in patients.
The Health Checks programme represents a particular opportunity to identify those with high blood pressure, and to encourage better management of the risk. Identifying and effectively managing hypertension, along with optimal lipid management, is crucial to reducing the risk of heart attacks and strokes. This is a key component of the Core20PLUS5 programme, which aims to address health inequalities.
Key indicator: Hypertension QOF Prevalence (all ages)
Alcohol (Behavioural)
Most people who consume alcohol do so at lower risk levels, within the guidelines of safer alcohol use. It becomes an issue for individuals, their families and the wider community when people drink alcohol at levels above the guidelines, causing significant health, social and criminal justice problems.
Alcohol consumption has a wide range of health harms. It has been linked to over 60 medical conditions, including cardiovascular diseases, cancers of the digestive organs, breast cancer, depression, suicide, and fertility problems.
In England, alcohol misuse is the biggest risk factor for early mortality, ill health and disability in the 15 to 49 age group.
Key indicator: Alcohol Specific Mortality (persons, 1 year range)
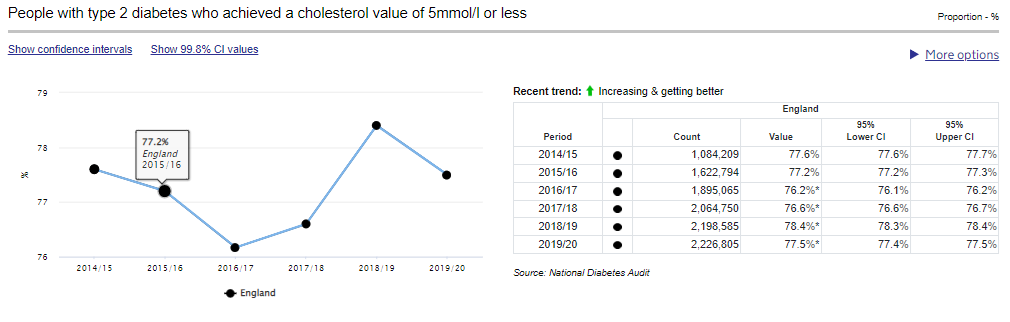
High LDL Cholesterol (Secondary)
Low-density lipoprotein (LDL) or ‘bad’ cholesterol is mainly caused by eating fatty food, not exercising enough, being overweight, smoking and drinking alcohol. It can also run in families. Too much cholesterol can block blood vessels. It makes heart problems or a stroke more likely. High cholesterol does not cause symptoms and can only be detected from a blood test. It can then be treated with behaviour change or medicine.
Key indicator: People with type 2 diabetes who achieved a cholesterol value of 5mmol/l or less
Low temperature (Environmental)
Low temperature is an environmental risk factor affected by the weather, and a major element in the higher incidence of disease and ‘winter pressures’ in the cold months. Its impact is greatest for those in draughty and cold homes. As a physiological response, hypothermia happens when the body temperature drops below 35 °C.
The risk of hypothermia is increased for those who do not wear enough clothes in cold weather, stay out in the cold too long, fall into cold water, have wet clothes and get cold, or live in a cold house. Older people living alone are particularly at risk. Fuel poverty can also contribute to these risks.
Key indicator: Fuel Poverty (low income, low energy efficiency methodology)
Diet low in whole grains (Behavioural)
Wholegrain varieties of starchy foods (and potatoes – particularly when eaten with their skin on) are good sources of fibre. Fibre is the name given to a range of substances found in the cell walls of vegetables, fruits, pulses and cereal grains. Fibre that cannot be digested helps other food and waste products to move through the gut.
Potato skins, wholegrain bread and breakfast cereals, brown rice, and wholewheat pasta are all good sources of this kind of fibre. Fibre can help keep bowels healthy, and encourage a feeling of fullness, making it less likely to eat too much. Wholegrain, wholemeal and brown breads also contain B vitamins, vitamin E, fibre and a wide range of minerals.
We do not have local data on consumption of wholegrain. Given its prominence in the list of risk factors, this may be an area for local research to help understand and action. Consumption of ‘five a day’ fruit and vegetables is often used as a proxy for quality of diet, more information can be found on our Living well page.
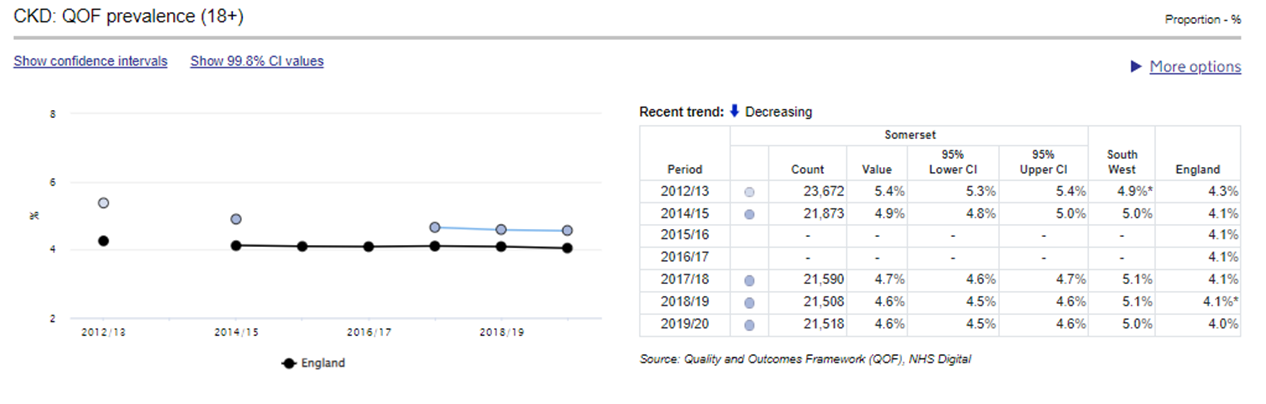
Kidney disfunction (Secondary)
Chronic kidney disease (CKD) is a long-term condition where the kidneys do not work as well as they should. It is a common condition often associated with getting older. It can affect anyone, but it’s more common in people who are black or of south Asian origin.
Chronic kidney disease (CKD) can get worse over time and eventually the kidneys may stop working altogether, but this is uncommon. Many people with Chronic kidney disease (CKD) are able to live long lives with the condition. There are usually no symptoms of kidney disease in the early stages. It may only be diagnosed in a blood or urine test for another reason and the results show a possible problem.
Chronic kidney disease (CKD) can be caused by a range of other risk factors, including high blood pressure which can put strain on the small blood vessels in the kidneys. It also can cause diabetes where too much blood glucose can damage the tiny filters in the kidneys, and high cholesterol which can cause a build-up of fatty deposits in the blood vessels supplying the kidneys, making it harder for them to work properly.
Occupational carcinogens (Environmental)
Occupational cancer may occur as a result of work involving direct exposure to a carcinogen or exposure to a carcinogen produced as part of a work process. There is usually a considerable amount of time (usually more than 10 years) between exposure to a carcinogen and the onset of any ill-health symptoms.
Carcinogens occur in many forms, they can be solids, liquids, vapours, gases, or dusts and can be breathed in, absorbed through the skin or swallowed. Asbestos, which can cause a range of asbestos related illnesses, is still particularly significant for those exposed before its ban in 1999.
We do not have local data on occupational carcinogens.